Rehabilitation following
|
Cartilage
1(2) 96–107 © The Author(s) 2010 Reprints and permission: sagepub.com/journalsPermissions.nav DOI: 10.1177/1947603510366029 http://cart.sagepub.com |
Kevin E. Wilk1, Leonard C. Macrina1, and Michael M. Reinold2
| Abstract Postoperative rehabilitation programs following articular cartilage repair procedures will vary greatly among patients and need to be individualized based on the nature of the lesion, the unique characteristics of the patient, and the type and detail of each surgical procedure. These programs are based on knowledge of the basic science, anatomy, and biomechanics of articular cartilage as well as the biological course of healing following surgery. The goal is to restore full function in each patient as quickly as possible by facilitating a healing response without overloading the healing articular cartilage. The purpose of this article is to overview the principles of rehabilitation following microfracture procedures of the knee. | |
Keywordsknee, rehabilitation, microfracture, arthroscopyIntroduction Articular cartilage defects of the knee are a common cause of pain and functional disability in orthopedics and sports medicine. The avascular nature of articular cartilage predis- poses the individual to progressive symptoms and degen- eration due to the extremely slow and oftentimes inability of the cartilage to heal.1-5 Nonoperative rehabilitation is frequently unsuccessful, and further treatment is required to alleviate symptoms. This presents a significant challenge for patients, particularly young and more active individuals who present without gross degenerative changes but rather focal cartilage defects. Postoperative rehabilitation programs will vary greatly among patients and are individualized based on lesion spe- cifics (size, depth, location, containment, quality of tissue), patient specifics (age, activities, goals, body mass index, general health), and surgical specifics (exact procedure, tis- sue involvement, concomitant surgeries). Thus, the devel- opment of an appropriate rehabilitation program is challenging and must be highly individualized to ensure successful outcomes. These programs are designed based on knowledge of the basic science, anatomy, and biome- chanics of articular cartilage as well as the biological course of healing following surgery. The goal is to restore full function in each patient as quickly as possible without overloading the healing articular cartilage. In this article, we will discuss the principles of rehabili- tation following the microfracture procedure and outline a course of treatment based on several fundamental principles. |
Rehabilitation Principles
Several principles exist that must be considered when designing a rehabilitation program following articular car- tilage repair procedures. These key principles have been designed based on understanding the basic science and mechanics of articular cartilage. Individualization The quality of each individual’s articular cartilage is the result of several factors, including age, body mass index, general health, nutrition, and history of previous injuries (Table 1). The composition of articular cartilage undergoes a gradual degeneration that results in a breakdown of tissue matrix and a reduction in the load-bearing capacity of the cartilage.6 The specific factors that contribute to this dete- rioration remain controversial, but it appears that age, obes- ity, poor nutrition, joint malalignment (such as a varus knee), history of injury (such as ligamentous or meniscal injury), and a history of repetitive impact loading (through 1 Champion Sports Medicine, American Sports Medicine Institute, Birmingham, Alabama, USA 2 Boston Red Sox, Major League Baseball, Boston, Massachusetts, and Department of Orthopedic Surgery, Division of Sports Medicine, Massachusetts General Hospital, Boston, Massachusetts, USA Corresponding Author: Leonard Macrina, MSPT, SCS, CSCS, Champion Sports Medicine, American Sports Medicine Institute, 805 St. Vincent’s Drive, Suite G100, Birmingham, AL 35205, USA Email: lenmac08@yahoo.com |
pagex
| Wilk et al. | 97 |
work or sport activities) may result in osteoarthritic changes.6 Thus, younger patients with isolated defects and relatively healthy surrounding articular cartilage oftentimes are able to progress their rehabilitation more rapidly than older individuals with more degenerative changes and less dense cartilage structure. Furthermore, the patient’s moti- vation and previous activity levels must be considered when determining the rehabilitation approach to ensure that the goals of each patient are addressed. The rehabilitation program should be individualized to the specific demands of each patient’s activities of daily living, work, and/or sport activities. There are also several variables to consider with regard to the lesion that may have a dramatic effect on the reha- bilitation process. Most importantly is the exact location of the lesion. Rehabilitation of lesions on a weightbearing surface of a femoral condyle must attempt to avoid deleteri- ous compressive forces and require a different approach than for lesions located within the trochlea or retrosurface of the patella, where excessive shear forces should be minimized. The size, depth, and containment of each lesion must also be considered. Lesions that are large, deep, or have poor containment with healthy surrounding articular cartilage may require a slower rehabilitation progression than smaller, shallower, or well-contained lesions. Finally, any concomitant procedures to address align- ment, stability, or meniscal function may also alter the rehabilitation program because of the need to protect other healing tissues. Create a Healing EnvironmentThe next principle of articular cartilage rehabilitation involves creating an environment that facilitates the healing | process while avoiding potentially deleterious forces to the repair site. Through animal studies, as well as closely monitoring the maturation of repair tissue in human patients via arthroscopic examination, the biological phases of maturation have been identified following several articular cartilage repair procedures.7-12 Knowledge of the healing and maturation process following these procedures will ensure that the repair tissue is gradually loaded and that excessive forces are not introduced too early in the healing process. Two of the most important aspects of rehabilitation of articular cartilage procedures are weightbearing restrictions and range-of-motion (ROM) limitations. Unloading and immobilization have been shown to be deleterious to heal- ing articular cartilage, resulting in proteoglycan loss and gradual weakening.13-16 Therefore, controlled weightbear- ing and ROM are essential to facilitate healing and prevent degeneration. This gradual progression has been shown to stimulate matrix production and improve the tissue’s mechanical properties.1,5,17 Controlled compression and decompression forces observed during weightbearing may nourish the articular cartilage and provide the necessary signals to the repair tis- sue to produce a matrix that will match the environmental forces.13,15,16 A progression of partial weightbearing with crutches is used to gradually increase the amount of load applied to the weightbearing surfaces of the joint. The use of a pool or aquatic therapy may also be beneficial to initi- ate gait training and lower extremity weightbearing exer- cises. The buoyancy of the water decreases the amount of weightbearing forces to approximately 25% of the indi- vidual’s body weight when submerged to the level of the axilla and 50% of the individual’s body weight when sub- merged to the level of the waist.18 A force platform is another useful tool during the early phases of rehabilitation when weightbearing is limited. This can be used to monitor the percentage of weightbear- ing on each extremity during exercises such as weight shifts, mini squats, and leg press (Fig. 1). The pool and force platforms may be used during early phases of rehabilitation to perform limited weightbearing activities designed to facilitate a normal gait pattern and enhance strength, proprioception, and balance. The authors believe that beginning controlled weightbearing activities during the early protective stage of healing is a critical com- ponent to the overall rehabilitation process. Although the return to functional activities will differ for each patient, it is our opinion that early initiation of controlled exercise ena- bles the individual to return to functional activities sooner than those who are immobilized and non-weightbearing. Passive range of motion (PROM) activities, such as continuous passive motion (CPM) machines or manual PROM performed by a rehabilitation specialist, are also performed immediately after surgery in a limited ROM to |
| 98 | Cartilage 1(2) |
nourish the healing articular cartilage and prevent the for- mation of adhesions.19-26 Motion exercises may assist in creating a smooth low frictional surface by sliding within the joint’s articular surface and may be an essential compo- nent to cartilage repair.19,20 It is the authors’ opinion that PROM is a safe and effective exercise to perform immedi- ately postoperatively, with minimal disadvantageous shear or compressive forces, if performed with patient relaxation. This ensures that muscular contraction does not create del- eterious compressive pressures or shearing forces. The use of CPM has been shown to enhance cartilage healing and long-term outcomes following articular carti- lage procedures.19-26 Comparing the outcomes of patients following microfracture procedures, Rodrigo et al.27 reported an 85% satisfactory outcome in patients using a CPM machine for 6 to 8 h per day for 8 wk as compared with a 55% satisfactory outcome in those patients who did not use a CPM machine. PROM can also be performed on a bike with adjustable pedals that can alter the available ROM (Unicam Corporation; Fig. 2). Biomechanics of the Knee Knowledge of the biomechanics of the tibiofemoral and patellofemoral joints is essential to appropriately design |
rehabilitation programs following articular cartilage repair procedures to ensure that exercises are selected and per- formed in a manner that does not cause deleterious forces to the repair site. Articulation between the femoral condyle and tibial plateau is constant throughout knee ROM. Near full knee extension, the anterior surface of each femoral condyle is in articulation with the middle aspect of the tibial plateau. With weightbearing, as the knee moves into greater flexion, the femoral condyles progressively roll posteriorly and slide anteriorly, causing the articulation to shift posteriorly on the femoral condyles and tibial plateaus.28,29 The articulation between the inferior margin of the patella and the trochlea begins at approximately 10° to 20° of knee flexion, depending on the size of the patella and the length of the patellar tendon.29 With knee flexion, the |
| Wilk et al. | 99 |
| |
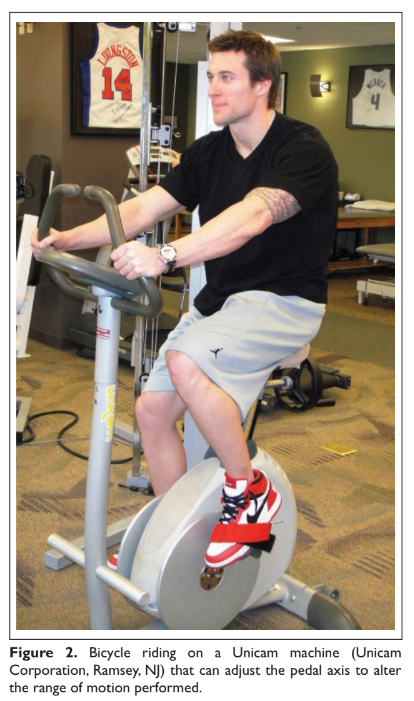
| contact area of the patellofemoral moves proximally. At 30° the area of patellofemoral contact (inferior facets) is approximately 2.0 cm2 . 30 The area of contact gradually increases as the knee is flexed. At 60° of knee flexion, the middle facet of the patella articulates with the trochlea. At 90° of knee flexion, the contact area increases up to 6.0 cm2 , and the superior facets are in contact with the femoral condyles.30 Using this knowledge of joint arthrokinematics, the rate of weightbearing, PROM, and exercise progression may be based on the exact location of the lesion (Fig. 3).31-34 For example, lesions on the posterior condyle may require the avoidance of exercise in deep knee flexion due to the roll- ing and sliding component of the articulation during deeper knee flexion. Furthermore, the rehabilitation program for lesions on the trochlea may include immediate partial weightbearing with a brace locked in full knee extension because the patella is not in contact with the trochlea in this position. Rehabilitation exercises are also altered based on the bio- mechanics of the knee to avoid excessive compressive or shearing forces. Although the exact ROM at which articula- tion of the lesion occurs is the most important factor to con- sider when designing the rehabilitation program, the amount | of compressive and shear forces observed at the joint also vary throughout the ROM. Exercises, such as seated knee extension, are commonly performed from 90° to 40° of knee flexion. This ROM provides the lowest amount of patel- lofemoral joint reaction forces while exhibiting the greatest amount of patellofemoral contact area.30,35,36 Weightbearing exercises such as the leg press, vertical squats, lateral step- ups, and wall squats are performed initially from 0° to 30°, where tibiofemoral and patellofemoral joint reaction forces are lower.30,35,36 Clinically, we begin these exercises using a leg press machine, rather than the vertical mini-squat, because of the better ability to control the amount of weight applied to the lower extremities. As the repair site heals and patient symptoms subside, the ROMs in which exercises are performed are progressed to allow greater muscle strength- ening over a greater ROM. Exercises are progressed based on the patient’s subjective reports of symptoms (pain, clicking, etc.) and the clinical assessment of increased swelling and crepitation. Reduction of Pain and Effusion Patients often exhibit pain and effusion following the microfracture procedure. Numerous authors have reported |
| 100 | Cartilage 1(2) |
| |
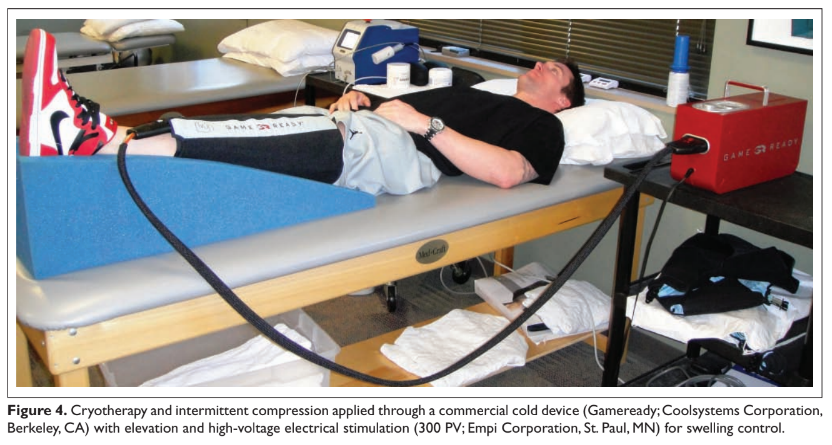
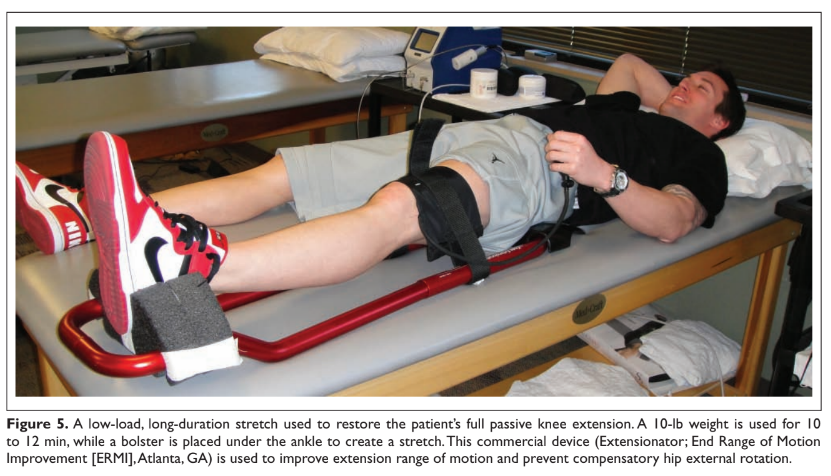
| a progressive decrease in volitional quadriceps activity as the knee exhibits increased pain and distention.37-40 Therefore, reduction in knee joint pain and swelling is cru- cial to minimize this reflex inhibition and restore normal quadriceps activity. Furthermore, any increase in intra- articular joint temperature has been shown to stimulate proteoglytic enzyme activity, which has a detrimental effect on articular cartilage.33,41 Treatment options for swelling reduction include cryo- therapy, elevation, high-voltage stimulation, and joint com- pression through the use of a knee sleeve or compression wrap (Fig. 4). Patients presenting with chronic joint effusion may also benefit from a knee sleeve or compression wrap to apply constant pressure while performing everyday activities. Pain can be reduced through the use of cryotherapy, transcutaneous electrical nerve stimulation, and analgesic medication. Immediately following injury or surgery, the use of a commercial cold wrap can be extremely beneficial. PROM may also provide neuromodulation of pain during acute or exacerbated conditions.24 Restore Soft-Tissue Balance One of the most important aspects of articular cartilage rehabilitation involves the avoidance of arthrofibrosis. This is achieved through the restoration of full passive knee extension, patellar mobility, and soft-tissue flexibility of the knee and entire lower extremity. The inability to fully | extend the knee results in abnormal joint arthrokinematics and subsequent increases in patellofemoral and tibiofemo- ral joint contact pressure, increased strain on the quadriceps muscle, and muscular fatigue.42 Therefore, a drop-lock postoperative knee brace locked into 0° of extension is used during ambulation, and PROM out of the brace is per- formed immediately following surgery. The goal is to achieve at least 0° of knee extension within the first few days following surgery. Specific exercises to be performed include manual PROM exercises applied by the rehabilitation specialist, supine hamstring stretches with a wedge under the heel, and gastrocnemius stretching with a towel. Overpressure of 2.7 to 5.4 kg (6 to 12 lb) may be used for a low-load, long-duration stretch as needed to achieve full extension (Fig. 5). Modalities such as moist heat and ultra- sound may also be applied to facilitate greater ROM improve- ments before and/or during these stretching techniques.43,44 The loss of patellar mobility following surgery may be due to various reasons including excessive scar tissue adhe- sions from the incision anteriorly, as well as along the medial and lateral aspects of the knee. The loss of patellar mobility may result in ROM complications and difficulty recruiting quadriceps contraction. Patellar mobilizations in the medial-lateral and superior-inferior directions are per- formed by the rehabilitation specialist and independently by the patient during the home exercise program. Soft-tissue flexibility and pliability are also important for the entire lower extremity. Soft-tissue mobilization and |
| Wilk et al. | 101 |
| |
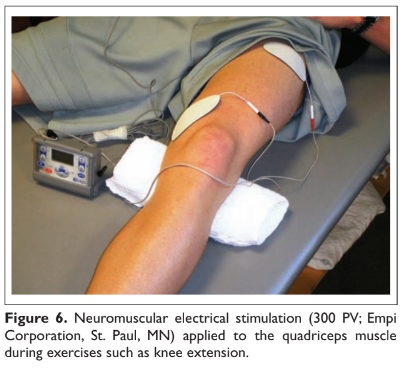
| scar management are performed to prevent the develop- ment of adhesions around the anterior, medial, and lateral aspects of the knee. In addition, flexibility exercises are performed for the entire lower extremity, including the hamstrings, hip, and calf musculature. As ROM improves and the lesion begins to heal, quadriceps stretching may also be performed as tolerated by the patient. Restoring Muscle Function Because of the inhibition of the quadriceps muscle second- ary to pain and effusion, electrical muscle stimulation and biofeedback are often incorporated with therapeutic exer- cises to facilitate the active contraction of the quadriceps musculature in the acute stage of rehabilitation. The use of electrical stimulation and biofeedback appears to facilitate the return of muscle activation.45,46 Clinically, we use electri- cal stimulation immediately following surgery while per- forming isometric and isotonic exercises such as quadriceps sets, straight leg raises, hip adduction and abduction, and knee extensions (Fig. 6). Electrical stimulation is used when the patient presents acutely with the inability to activate the quadriceps in an attempt to recruit a maximum amount of muscle fibers during active contraction and may also be used throughout the rehabilitation process. Once independent muscle activation is present, biofeedback may be used to facilitate further neuromuscular activation of the quadriceps. |
Exercises that strengthen the entire lower extremity, such as machine weights and weightbearing exercises, may be included as the patient progresses to more advanced phases of rehabilitation. It is important not to concentrate solely on the quadriceps. Furthermore, the importance of incorporating core stability exercises cannot be over- looked. Training of the trunk, hip, and ankle musculature is |
| 102 | Cartilage 1(2) |
|
emphasized to assist in controlling the production and dis-
sipation of forces in the knee.
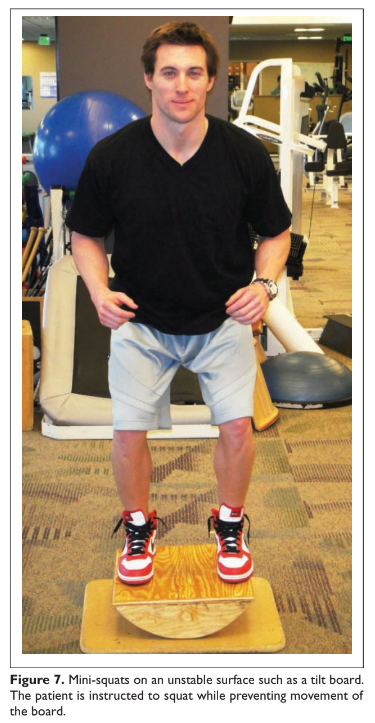
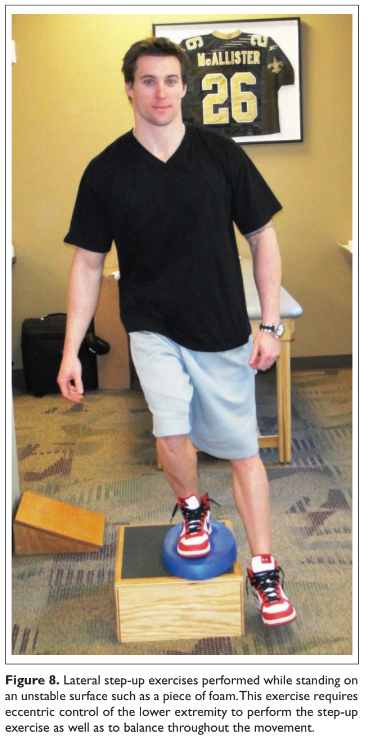
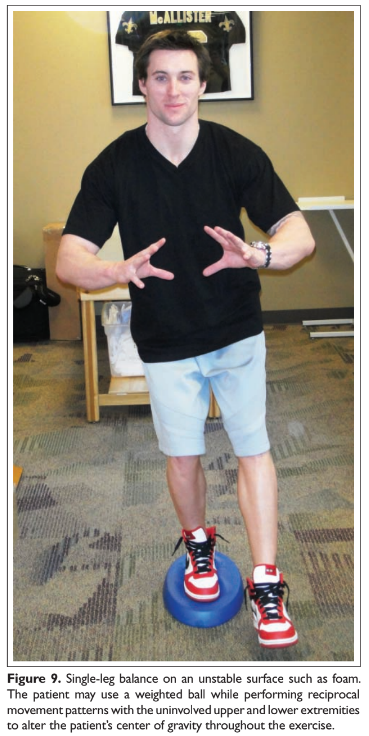
Enhance Proprioception and Neuromuscular Control Proprioceptive and neuromuscular control drills of the lower extremities should be included to restore dynamic stabilization of the knee joint postoperatively. Proprioceptive deficits have been noted in the injured and postoperative knee.47,48 Specific drills initially include weight shifting side to side, weight shifting diagonally, mini-squats, and mini-squats on an unstable surface such as a tilt or balance board (Fig. 7). Perturbations can be added to challenge the neuromuscular system, as can additional exercises includ- ing lunges, step-ups, and balance onto unstable surfaces (Figs. 8 and 9). Controlling the Application of Loads The next principle of rehabilitation involves gradually increasing the amount of stress applied to the injured knee as the patient returns to functional activities. This progres- sion is used to provide a healthy stimulus for healing carti- lage tissues while ensuring that forces are gradually applied without causing damage. Common clinical signs that a patient may be progressing too quickly and overloading the healing tissue are joint line pain and effusion. This should be monitored throughout the rehabilitation process. In addition, patients may benefit from the use of orthotics, insoles, and bracing to alter the applied loads on the articular cartilage during functional activities. These devices are used to avoid excessive forces by unloading the area of the knee where the lesion is located. Unloading braces are often used for patients with subtle uncorrected abnormal alignments (such as genu varum), patients with large or uncontained lesions, as well as in the presence of concomitant osteotomies and meniscal allografts (Fig. 10). Team Communication Communication between the surgeon and therapist is essen- tial to determine the accurate rate of progression based on the location of the lesion, size of the lesion, tissue quality of the patient, and the addition of concomitant surgical procedures. Also, communication between the medical team and patient is essential to provide the patient with education regarding the avoidance of deleterious forces as well as improving the patient’s compliance with precau- tions. Oftentimes, a preoperative physical therapy evalua- tion may be useful to mentally and physically prepare the patient for the articular cartilage procedure and postopera- tive rehabilitation. |
Rehabilitation following Microfracture Procedure Microfracture The microfracture procedure is a form of marrow stimula- tion, similar in concept to the chondroplasty procedure.49-51 A sharp awl is used arthroscopically through one of the portals, and a mallet is used to impact the awl into the subchondral bone and thus generate bleeding from the bone. This procedure is also referred to as “picking” because of its nature. Holes are created at regular intervals |
| Wilk et al. | 103 |
until the entire defect has been addressed. The penetration of the subchondral bone eventually creates fibrocartilagen- ous tissue that covers the cartilage lesion.49-51 The rehabilitation progression is designed based on the 4 biological phases of cartilage maturation: proliferation, transitional, remodeling, and maturation.7,8,10-12,41,52-54 The duration of each phase will vary depending on the lesion, patient, and the specifics of the surgery discussed previ- ously; however, the concepts of each phase are consistent. The following is an overview of the general rehabilitation process during each of the 4 phases. |
Phase 1: Proliferation Phase The 1st phase of cartilage healing requires protection of the repair and typically involves the first 4 to 6 wk following surgery.7,8,10-12,41,52-54 During this phase, the initial healing process begins, and it is imperative to decrease swelling, gradually restore PROM and weightbearing, and enhance volitional control of the quadriceps. Gradual PROM and controlled partial weightbearing will help to nurture the cartilage through diffusion of syno- vial fluid as well as provide the proper stimulus for the cells |
| 104 | Cartilage 1(2) |

to produce specific matrix markers.1,5,13,14,16,17 Individuals begin with partial weightbearing activities using crutches, and progressive loading exercises are used to gradually increase the amount of load applied to the weightbearing surfaces of the joint. The use of a pool or aquatic therapy may be beneficial for gait training and lower extremity exercises once the incisions are well healed. PROM exercises, performed by a rehabilitation special- ist or CPM machines, are also performed immediately after surgery to nourish the healing articular cartilage and pre- vent the formation of adhesions.19,20,24-27 The use of CPM typically begins 6 to 8 h following surgery and is per- formed for at least 2 to 3 wk, with recommended use up to 6 to 8 wk.27,55 A CPM should be used throughout the day for a total of 6 to 8 h.27,55 The patient is also instructed to perform active-assisted ROM frequently throughout the | day. Patellar mobilization, soft-tissue mobilization, and soft-tissue flexibility exercises are also performed to mini- mize scar tissue formation and avoid loss of motion. Early strengthening exercises are performed to restore volitional quadriceps control and neuromuscular control, through the use of concomitant electrical stimulation.45,46 Exercises performed during this phase are limited based on the specific weightbearing status of each patient. These typically include quadriceps sets, straight leg raises, and basic proprioception exercises such as weight shifting. Phase 2: Transition Phase This phase typically consists of weeks 4 through 12 post- surgery.7,8,10-12,41,52-54 The repair tissue at this point is gain- ing strength, which will allow for the progression of rehabilitation exercises. During this phase, the patient progresses from partial to full weightbearing while full ROM and soft-tissue flexibility is achieved. Continued maturation of the repair tissue is fostered through higher level functional and motion exercises. It is during this phase that patients typically resume most normal activities of daily living. The rehabilitation program will gradually progress strengthening activities to include machine weights and weightbearing exercises, such as leg press, front lunges, wall slides, and lateral step-ups, as the patient’s weightbearing status returns to normal. The progression of weightbearing activities and ROM restoration involves the gradual advancement of activities to facilitate healing and avoid postsurgical complications. Common complications include motion restrictions and scar tissue formation. Furthermore, an overaggressive approach early within the rehabilitation program may result in increased pain, inflammation, or effusion, as well as graft damage. Progression is controlled for strengthening exercises, proprioception training, neuromuscular control drills, and functional drills. For example, exercises such as weight shifts and lunges are progressed from straight plane anterior-posterior or medial-lateral directions to involve multiplane and rotational movements. Exercises using 2 lower extremities, such as leg press and balance activities, are progressed to single lower extremity exercises. Thus, the progression through the postoperative rehabilitation program involves a gradual progression of applied and functional stresses to provide a healthy stimulus for healing tissues without causing damage. Phase 3: Remodeling Phase This phase generally takes place from 3 mo to 6 mo post- operatively.7,8,10-12,41,52-54 During this phase, there is a con- tinuous remodeling of tissue into a more organized structure that is increasing in strength and durability.7,8,10-12,41,52-54 As |
| Wilk et al. | 105 |
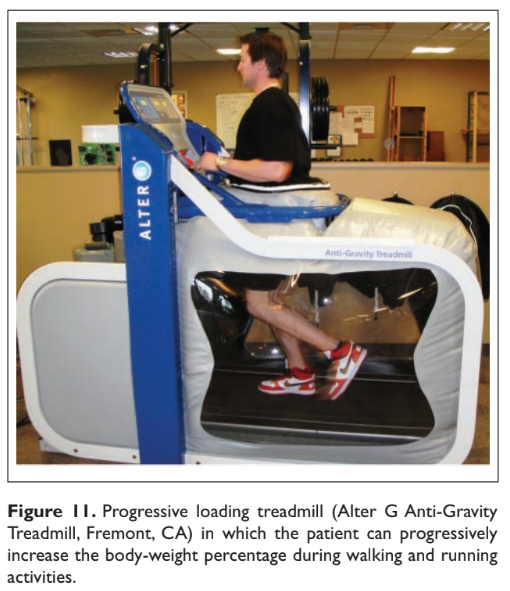
the tissue becomes firmer and integrated, it allows for more functional training activities to be performed. At this point, the patient typically notes improvement of symptoms and has normal ROM. The patient is encouraged to continue with his or her rehabilitation program independently to maximize strength and flexibility. Low- to moderate-impact activities such as bicycle riding, golfing, and recreational walking may often be gradually incorporated (Figure 11). Phase 4: Maturation Phase The final phase begins in the range of 4 mo to 6 mo and can last up to 15 to 18 mo postsurgery.7,8,10-12,41,52-54 It is during this phase that the repair tissue reaches its full maturation. The duration of this phase varies based on several factors, such as lesion size and location and the specific surgical procedure performed. The patient will gradually return to full premorbid activities as tolerated. Impact loading activ- ities are gradually introduced. A return to athletic activities is determined based on the unique presentation of each patient. A return to competitive athletics has been docu- mented for microfracture, with good outcomes often expected.49-51,56-61 Conclusion The rehabilitation process following articular cartilage repair procedures is vital to the long-term success and functional | outcome of these patients. The rehabilitation programs dis- cussed are based on our current understanding of articular cartilage and the natural healing response observed follow- ing articular cartilage repair procedures. Rehabilitation is based on several key principles used to facilitate the repair process by creating a healing environment while avoiding deleterious forces that may overload the healing tissue. It must also consider any concomitant surgery performed. The basic principles outlined in this article may be applied and integrated as our understanding and clinical use of this procedure improve. Declaration of Conflicting Interests The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article. Funding The authors received no financial support for the research and/or authorship of this article. References 1. Buckwalter JA. Articular cartilage: injuries and potential for healing. J Orthop Sports Phys Ther. 1998 Oct;28(4):192-202. 2. Buckwalter JA. Articular cartilage injuries. Clin Orthop Relat Res. 2002 Sep;402:21-37. 3. Buckwalter JA. Integration of science into orthopaedic prac- tice: implications for solving the problem of articular cartilage repair. J Bone Joint Surg Am. 2003;85-A(suppl 2):1-7. 4. Buckwalter JA, Mankin HJ. Articular cartilage: degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect. 1998;47:487-504. 5. Buckwalter JA, Mankin HJ. Articular cartilage: tissue design and chondrocyte-matrix interactions. Instr Course Lect. 1998;47:477-86. 6. Cohen NP, Foster RJ, Mow VC. Composition and dynamics of articular cartilage: structure, function, and maintaining healthy state. J Orthop Sports Phys Ther. 1998 Oct;28(4):203-15. 7. Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L. Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med. 1994 Oct 6;331(14):889-95. 8. Brittberg M, Nilsson A, Lindahl A, Ohlsson C, Peterson L. Rabbit articular cartilage defects treated with autolo- gous cultured chondrocytes. Clin Orthop Relat Res. 1996 May;326:270-83. 9. Brittberg M, Winalski CS. Evaluation of cartilage injuries and repair. J Bone Joint Surg Am. 2003;85-A(suppl 2):58-69. 10. Grande DA, Pitman MI, Peterson L, Menche D, Klein M. The repair of experimentally produced defects in rabbit articular cartilage by autologous chondrocyte transplantation. J Orthop Res. 1989;7(2):208-18. 11. Peterson L, Brittberg M, Kiviranta I, Akerlund EL, Lindahl A. Autologous chondrocyte transplantation: biomechanics and long-term durability. Am J Sports Med. 2002 Jan-Feb;30(1):2-12. |
| Wilk et al. | 99 |
| 12. Peterson L, Minas T, Brittberg M, Nilsson A, Sjogren-Jansson E, Lindahl A. Two- to 9-year outcome after autologous chon- drocyte transplantation of the knee. Clin Orthop Relat Res. 2000 May;374:212-34. 13. Behrens F, Kraft EL, Oegema TR Jr. Biochemical changes in articular cartilage after joint immobilization by casting or external fixation. J Orthop Res. 1989;7(3):335-43. 14. Haapala J, Arokoski J, Pirttimaki J, Lyyra T, Jurvelin J, Tammi M, et al. Incomplete restoration of immobilization induced soft- ening of young beagle knee articular cartilage after 50-week remobilization. Int J Sports Med. 2000 Jan;21(1):76-81. 15. Haapala J, Arokoski JP, Ronkko S, Agren U, Kosma VM, Lohmander LS, et al. Decline after immobilisation and recov- ery after remobilisation of synovial fluid IL1, TIMP, and chondroitin sulphate levels in young beagle dogs. Ann Rheum Dis. 2001 Jan;60(1):55-60. 16. Vanwanseele B, Lucchinetti E, Stussi E. The effects of immobili- zation on the characteristics of articular cartilage: current concepts and future directions. Osteoarthr Cart. 2002 May;10(5):408-19. 17. Waldman SD, Spiteri CG, Grynpas MD, Pilliar RM, Hong J, Kandel RA. Effect of biomechanical conditioning on car- tilaginous tissue formation in vitro. J Bone Joint Surg Am. 2003;85-A(suppl 2):101-5. 18. Harrison RA, Hillman M, Bulstrode S. Loading of the limb when walking partially immersed. Physiotherapy. 1992;78:164-6. 19. Salter RB. The biologic concept of continuous passive motion of synovial joints: the first 18 years of basic research and its clinical application. Clin Orthop Relat Res. 1989 May;242:12-25. 20. Salter RB. The physiologic basis of continuous passive motion for articular cartilage healing and regeneration. Hand Clin. 1994 May;10(2):211-9. 21. Salter RB. History of rest and motion and the scientific basis for early continuous passive motion. Hand Clin. 1996 Feb;12(1):1-11. 22. Salter RB. Continuous passive motion: from origination to research to clinical applications. J Rheumatol. 2004 Nov;31(11):2104-5. 23. Salter RB, Bell RS, Keeley FW. The protective effect of con- tinuous passive motion in living articular cartilage in acute septic arthritis: an experimental investigation in the rabbit. Clin Orthop Relat Res. 1981 Sep;159:223-47. 24. Salter RB, Hamilton HW, Wedge JH, et al. Clinical application of basic research on continuous passive motion for disorders and injuries of synovial joints: a preliminary report of a feasi- bility study. J Orthop Res. 1984;1(3):325-42. 25. Salter RB, Simmonds DF, Malcolm BW, Rumble EJ, Mac- Michael D, Clements ND. The biological effect of continu- ous passive motion on the healing of full-thickness defects in articular cartilage: an experimental investigation in the rabbit. J Bone Joint Surg Am. 1980 Dec;62(8):1232-51. 26. Williams JM, Moran M, Thonar EJ, Salter RB. Continuous passive motion stimulates repair of rabbit knee articular car- tilage after matrix proteoglycan loss. Clin Orthop Relat Res. 1994 Jul;304:252-62. | 27. Rodrigo JJ, Steadman JR, Sillman JF. Improvement of full- thickness chondral defect healing in the human knee after debridement and microfracture using continuous passive motion. Am J Knee Surg. 1994;7:109-16. 28. Iwaki H, Pinskerova V, Freeman MA. Tibiofemoral move- ment 1: the shapes and relative movements of the femur and tibia in the unloaded cadaver knee. J Bone Joint Surg Br. 2000 Nov;82(8):1189-95. 29. Martelli S, Pinskerova V. The shapes of the tibial and femo- ral articular surfaces in relation to tibiofemoral movement. J Bone Joint Surg Br. 2002 May;84(4):607-13. 30. Hungerford DS, Barry M. Biomechanics of the patellofemoral joint. Clin Orthop Relat Res. 1979 Oct;144:9-15. 31. Blankevoort L, Kuiper JH, Huiskes R, Grootenboer HJ. Artic- ular contact in a three-dimensional model of the knee. J Bio- mech. 1991;24(11):1019-31. 32. Fujikawa K, Seedhom BB, Wright V. Biomechanics of the patello-femoral joint. Part I: a study of the contact and the congruity of the patello-femoral compartment and movement of the patella. Eng Med. 1983 Jan;12(1):3-11. 33. Goodfellow J, Hungerford DS, Woods C. Patello-femoral joint mechanics and pathology. 2. Chondromalacia patellae. J Bone Joint Surg Br. 1976 Aug;58(3):291-9. 34. Goodfellow J, Hungerford DS, Zindel M. Patello-femoral joint mechanics and pathology. 1. Functional anatomy of the patello- femoral joint. J Bone Joint Surg Br. 1976 Aug;58(3):287-90. 35. Huberti HH, Hayes WC. Patellofemoral contact pressures: the influence of q-angle and tendofemoral contact. J Bone Joint Surg Am. 1984 Jun;66(5):715-24. 36. Steinkamp LA, Dillingham MF, Markel MD, Hill JA, Kaufman KR. Biomechanical considerations in patellofemoral joint rehabilitation. Am J Sports Med. 1993 May-Jun;21(3):438-44. 37. Horvath SM, Hollander JL. Intra-articular temperature as a measure of joint reaction. J Clin Invest. 1949;28:469-73. 38. Osbahr DC, Cawley PW, Speer KP. The effect of continuous cryotherapy on glenohumeral joint and subacromial space temperatures in the postoperative shoulder. Arthroscopy. 2002 Sep;18(7):748-54. 39. Spencer JD, Hayes KC, Alexander IJ. Knee joint effusion and quadriceps reflex inhibition in man. Arch Phys Med Rehabil. 1984 Apr;65(4):171-7. 40. Young A, Stokes M, Shakespeare DT. The effect of intra-artic- ular bupivicaine on quadriceps inhibition after meniscectomy. Med Sci Sports Exerc. 1983;15(2):154. 41. Hangody L, Kish G, Karpati Z. Autogenous osteochondral graft technique for replacing knee cartilage defects in dogs. Orthop Int. 1997;5:175-81. 42. Perry J, Antonelli D, Ford W. Analysis of knee-joint forces during flexed-knee stance. J Bone Joint Surg Am. 1975 Oct;57(7):961-7. 43. Knight CA, Rutledge CR, Cox ME, Acosta M, Hall SJ. Effect of superficial heat, deep heat, and active exercise warm-up on the extensibility of the plantar flexors. Phys Ther. 2001 Jun;81(6):1206-14. |
| Wilk et al. | 107 |
| 44. Robertson VJ, Ward AR, Jung P. The effect of heat on tissue extensibility: a comparison of deep and superficial heating. Arch Phys Med Rehabil. 2005 Apr;86(4):819-25. 45. Delitto A, Rose SJ, McKowen JM, Lehman RC, Thomas JA, Shively RA. Electrical stimulation versus voluntary exercise in strengthening thigh musculature after anterior cruciate liga- ment surgery. Phys Ther. 1988 May;68(5):660-3. 46. Snyder-Mackler L, Delitto A, Bailey SL, Stralka SW. Strength of the quadriceps femoris muscle and functional recovery after reconstruction of the anterior cruciate ligament: a prospective, randomized clinical trial of electrical stimulation. J Bone Joint Surg Am. 1995 Aug;77(8):1166-73. 47. Friden T, Roberts D, Ageberg E, Walden M, Zatterstrom R. Review of knee proprioception and the relation to extremity function after an anterior cruciate ligament rupture. J Orthop Sports Phys Ther. 2001 Oct;31(10):567-76. 48. Roberts D, Friden T, Stomberg A, Lindstrand A, Moritz U. Bilateral proprioceptive defects in patients with a unilat- eral anterior cruciate ligament reconstruction: a comparison between patients and healthy individuals. J Orthop Res. 2000 Jul;18(4):565-71. 49. Steadman JR, Miller BS, Karas SG, Schlegel TF, Briggs KK, Hawkins RJ. The microfracture technique in the treatment of full-thickness chondral lesions of the knee in National Foot- ball League players. J Knee Surg. 2003 Apr;16(2):83-6. 50. Steadman JR, Rodkey WG, Briggs KK. Microfracture to treat full-thickness chondral defects: surgical technique, rehabilita- tion, and outcomes. J Knee Surg. 2002 Summer;15(3):170-6. 51. Steadman JR, Rodkey WG, Rodrigo JJ. Microfracture: surgi- cal technique and rehabilitation to treat chondral defects. Clin Orthop Relat Res. 2001 Oct;391(suppl):S362-9. 52. Frisbie DD, Oxford JT, Southwood L, et al. Early events in cartilage repair after subchondral bone microfracture. Clin Orthop Relat Res. 2003 Feb;407:215-27. 53. Hangody L, Kish G, Karpati Z, Szerb I, Udvarhelyi I. Arthroscopic autogenous osteochondral mosaicplasty for the | treatment of femoral condylar articular defects: a prelimi- nary report. Knee Surg Sports Traumatol Arthrosc. 1997;5(4): 262-7. 54. Nam EK, Makhsous M, Koh J, Bowen M, Nuber G, Zhang LQ. Biomechanical and histological evaluation of osteochon- dral transplantation in a rabbit model. Am J Sports Med. 2004 Mar;32(2):308-16. 55. Reinold MM, Wilk KE, Macrina LC, Dugas JR, Cain EL. Cur- rent concepts in the rehabilitation following articular cartilage repair procedures in the knee. J Orthop Sports Phys Ther. 2006 Oct;36(10):774-94. 56. Asik M, Ciftci F, Sen C, Erdil M, Atalar A. The microfracture technique for the treatment of full-thickness articular carti- lage lesions of the knee: midterm results. Arthroscopy. 2008 Nov;24(11):1214-20. 57. Gobbi A, Nunag P, Malinowski K. Treatment of full thick- ness chondral lesions of the knee with microfracture in a group of athletes. Knee Surg Sports Traumatol Arthrosc. 2005 Apr;13(3):213-21. 58. Riyami M, Rolf C. Evaluation of microfracture of traumatic chondral injuries to the knee in professional football and rugby players. J Orthop Surg Res. 2009;4:13. 59. Solheim E, Oyen J, Hegna J, Austgulen OK, Harlem T, Strand T. Microfracture treatment of single or multiple articular car- tilage defects of the knee: a 5-year median follow-up of 110 patients. Knee Surg Sports Traumatol Arthrosc. Epub ahead of print, 29 October 2009. 60. Steadman JR, Briggs KK, Rodrigo JJ, Kocher MS, Gill TJ, Rodkey WG. Outcomes of microfracture for traumatic chon- dral defects of the knee: average 11-year follow-up. Arthros- copy. 2003 May-Jun;19(5):477-84. 61. Cerynik DL, Lewullis GE, Joves BC, Palmer MP, Tom JA. Outcomes of microfracture in professional basketball play- ers. Knee Surg Sports Traumatol Arthrosc. 2009 Sep;17(9): 1135-9. |